by Anh Luu
The heart is an incredible four-chambered machine that beats 60-100 times per minute to keep blood circulating and feeding oxygen to the rest of the body. The top two chambers are called atria, and the bottom two ventricles. For the heart to function properly, it needs not only healthy cells and a stable structure, but also a working electrical system that tells it how fast or how slow to beat. The atria squeeze first, followed by the ventricles. This ensures that blood can flow from the atria to the ventricles, and then from the ventricles to the body in a regular manner (Figure 1).
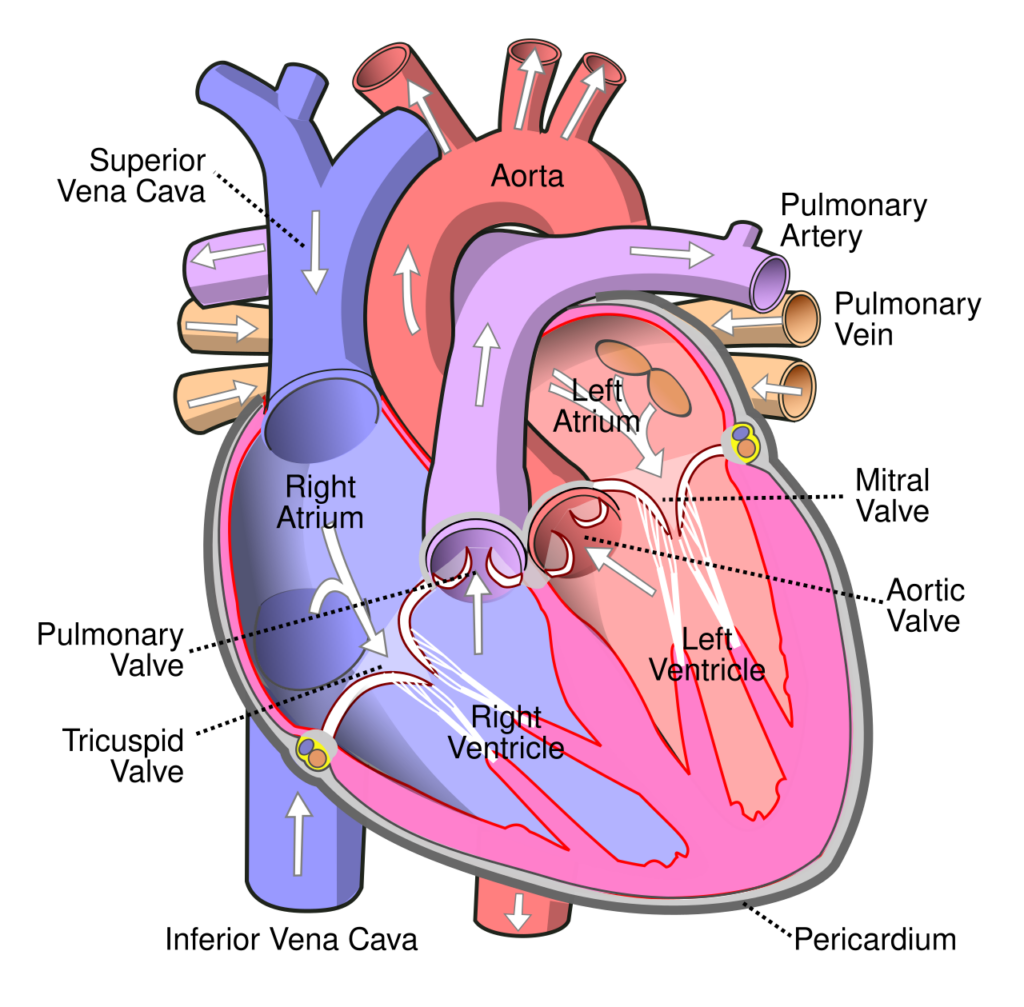
Figure 1. Blood flow in the heart (white arrows). Image source: Wikimedia
A heart arrhythmia means the heart is not beating with the correct timing. This can come from abnormal pacemaker cells (the starting point) or other heart muscle cells. One of the most common forms of arrhythmia is atrial fibrillation (Afib), characterized by very fast, chaotic heartbeats as the atria fail to contract properly (Figure 2). This greatly disrupts the regular blood flow, and the heart will fail to meet the body’s demand, or even worse, the blood may clot and cause a stroke if that clot ends up in the brain.
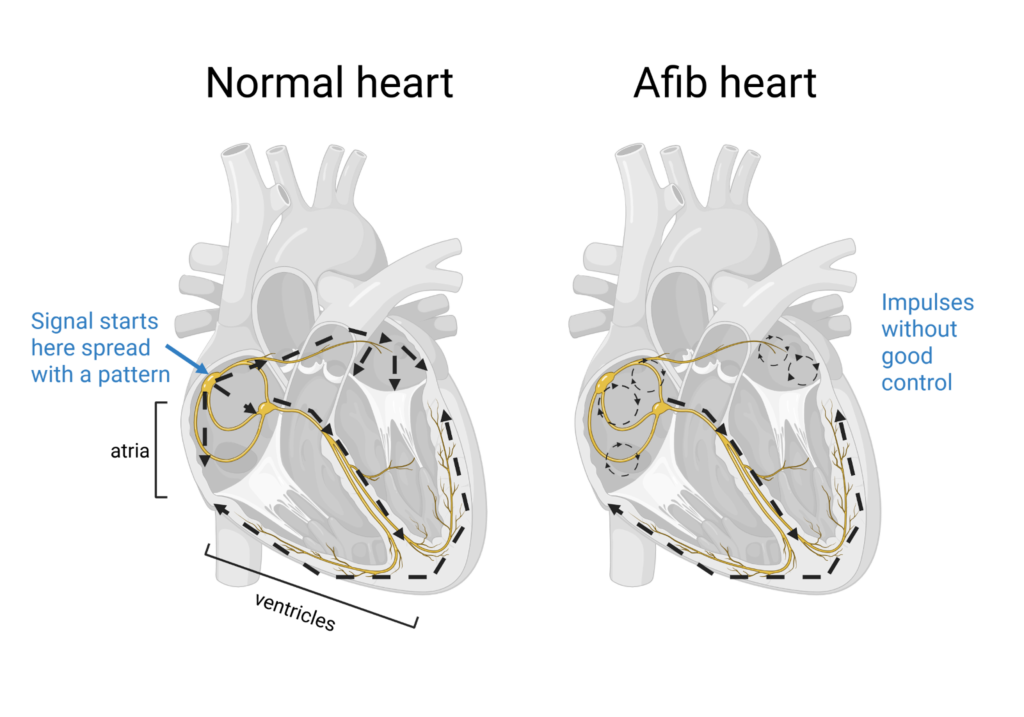
Figure 2. Cardiac conduction system in a normal heart and a heart with Afib. Normal impulses follow from the atrium to the ventricle. In Afib, the impulses in the atria are irregular and may circle within the atria. Image created by BioRender.
The cornerstones of current Afib treatment include lifestyle changes (i.e., cutting back on alcohol) and controlling the heart’s rhythm and rate with medications. In some cases, patients will undergo ablation, a procedure in which physicians deliberately “zap” erratic or chaotic heart cells so they don’t disrupt the electrical current flowing through healthy, functional cells. Some patients who have an extra-slow heartbeat due to a heart disease other than Afib will also get a pacemaker (check out this cool movie from the American Heart Association). This is a small device that generates electrical signals to artificially set a steady heart rate: taking over for the heart’s dysfunctional pacemaker cells. Additionally, since Afib is known to increase the risk for blood clots and stroke, Afib patients take blood thinner drugs to lower their risk and prevent serious complications.
Afib could be influenced by genetics. For example, mutations in genes such as KCNQ1, TBX5, or NKX2-5 can lead to cardiac conduction abnormalities and AFib. Currently, there are no standard treatments that address the genetic component of this disorder, leaving plenty of room for further research and drug development.

.svg){kind=link}