by Miraya Baid
In the 16th century, French military surgeon Ambroise Paré tended to soldiers whose legs had been blown off by cannon fire, many of whom insisted that their missing limbs were still attached. Paré’s observations mark the first recorded account of ‘phantom limbs,’ a phenomenon that affects roughly 60 to 80 percent of the 185,000 Americans who undergo amputation each year. A devastatingly large proportion of amputees experience chronic phantom pain, the clinical reality of which is evidenced by patient reports describing the amputated limb as being clenched into an irresolvable fist or nails cutting into a palm they cannot open.
“This fear was unbearable. It unwrapped who she was, as neatly as he’d unwound her bandage, leaving too much pain and ugliness exposed. Nerve endings; he’d said they were the problem [causing phantom pain in the amputated limb]. Things that cut off, that ended abruptly or died–like parents and marriages–kept hurting forever.”
– ‘Home Front’ by Kristin Hannah
Somatotopic Organization of the Primary Somatosensory Cortex
The perception of phantom limbs arises from activity in the primary somatosensory cortex, the brain region responsible for processing all somatic sensations, including touch, pain, temperature, and proprioception (sense of body position). It houses the brain’s internal map of the body. It was first charted in detail by Wilder Penfield through intraoperative cortical stimulation in the 1930s, who discovered that the topographic representation of the hands, face, and lips dwarfs that of the torso, and the genitals are improbably wedged next to the feet. This disproportionate and disorganized ‘sensory homunculus,’ translating to ‘little man’ in Latin, accounts for highly localized phantom-hand sensations; amputees can often feel individual phantom fingers flexing or curling. Phantom legs, by contrast, tend to produce more diffuse burning or cramping.
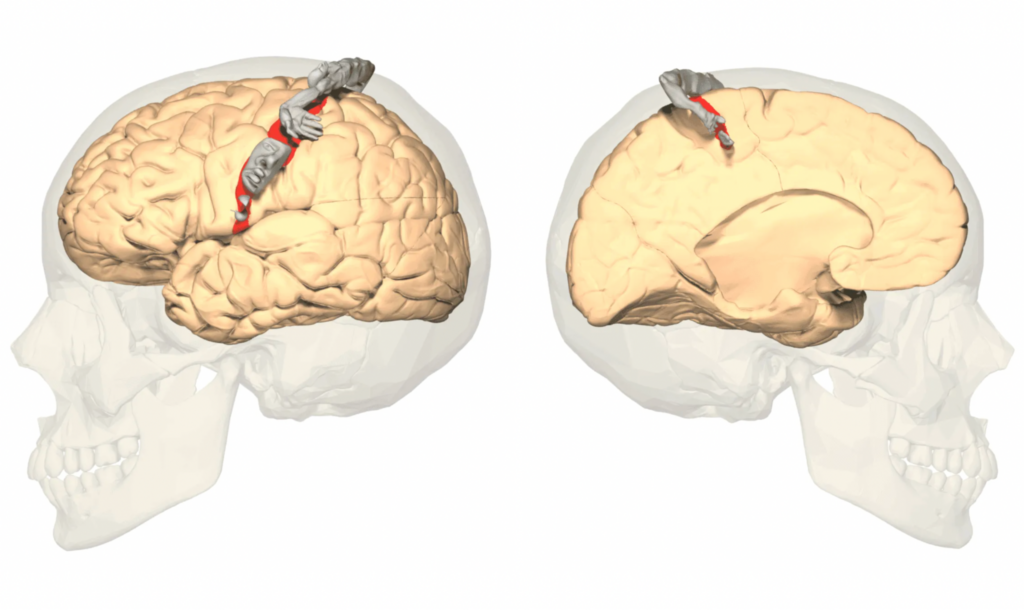
The position of the somatosensory cortex is situated in the postcentral gyrus of the parietal lobe. Image by Database Center for Life Science (DBCLS)/Anatomography, licensed under CC BY-SA 2.1 JP.
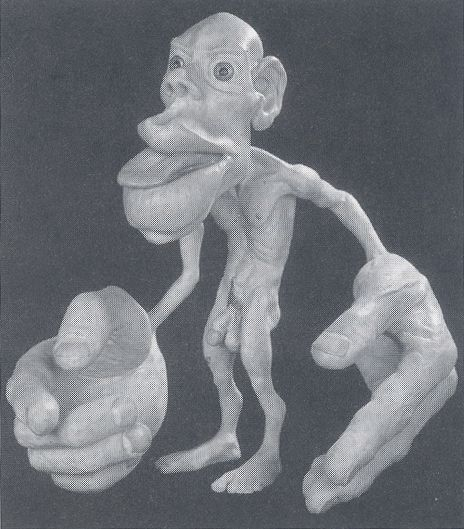
Cortical representation of the body in the brain, the homunculus (Penfield, 1950). Image by Ayacop, published in the public domain via Wikimedia Commons.
Neuroanatomical Substrate: Cortical Reorganization Following Deafferentation
In the 1990s, neuroscientist V. S. Ramachandran demonstrated that this somatotopic map is not a static wiring diagram, but a dynamic, experience-dependent structure that the brain continuously recalibrates against incoming sensory data. The maps are the body, as far as conscious experience is concerned, and the physical limb is merely one of several inputs that keep the map well-calibrated. After amputation, the cortical territory formerly devoted to the lost limb undergoes rapid and extensive reorganization: neighboring representations, typically the face and the upper arm in the case of a lost hand, expand into the deafferented zone within weeks. Tim Pons and colleagues showed this dramatically in macaques in 1991, and Herta Flor‘s group later demonstrated in human amputees that the magnitude of this remapping tracks linearly with the severity of phantom limb pain.
Phantom sensations arise because the brain’s model retains a representation of the missing limb, and cross-modal input from adjacent cortical zones gets misattributed to the ghost, a process called maladaptive neuroplasticity, producing referred sensations, spontaneous movement illusions, and often searing, treatment-resistant pain. Critically, if the last real sensation received from the limb was agonizing pain, as was presumably felt by Paré’s soldiers on the battlefield, the brain’s predictive machinery, deprived of corrective proprioceptive and tactile input, may continue to predict and hence experience the same agony indefinitely. This accounts for the finding that veterans who lose limbs to trauma report significantly higher rates of phantom pain than those who lose limbs to cancer or vascular disease.
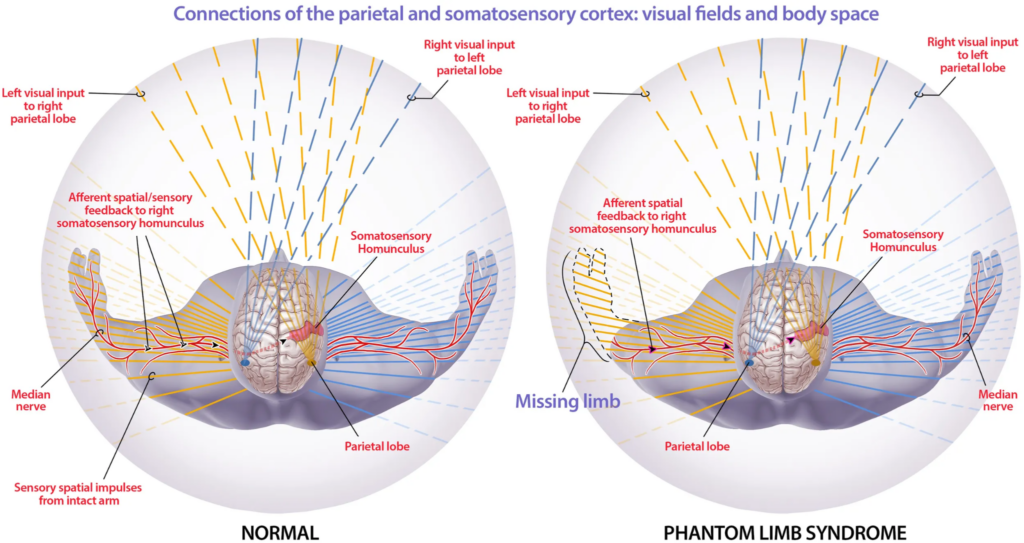
Intact sensorimotor circuits generate phantom sensations that conflict with visual input of the missing limb (Jerath, Crawford, & Barnes, 2015). Image by Michael Jensen, MSMI, CMI, published under CC BY 4.0.
In 1995, Ramachandran devised a simple but revolutionary treatment he termed the ‘mirror box,’ a device fitted with a vertical mirror such that when a patient places their intact arm into the box, the reflection creates the illusion that the missing limb has returned since the visual system registers bilateral movement. This strong, congruent sensory signal updates the brain’s internal model. Many patients report that a painfully clenched phantom fist unclenches for the first time in years. Their pain drops dramatically after mirror therapy, which has since become a standard, non-invasive intervention, though it does not work to absolve phantom limb pain for all patients.
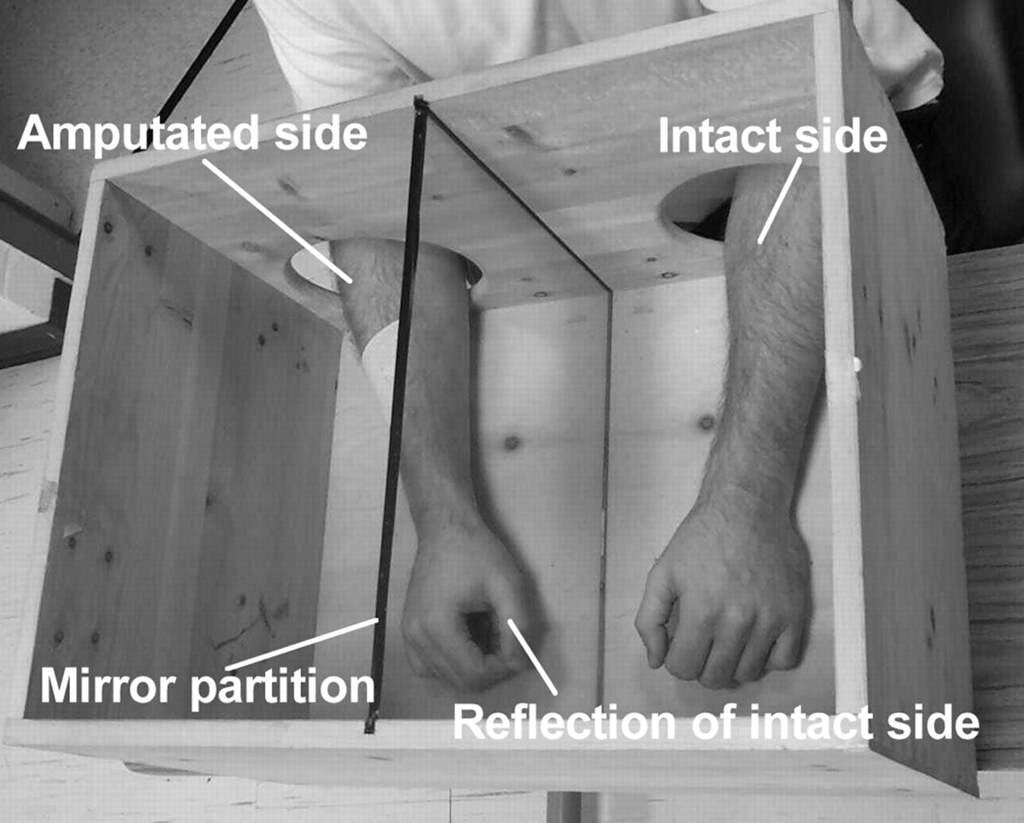
Example of a mirror-box used to provide visual feedback (Faure et al., 2019). Image by Edhubbard, published in the public domain.
The Body as Bayesian Inference
However, phantom limbs cannot be described in their completeness as sensory afterimages of an amputated limb. Remarkably, the phenomenon does not even require prior physical experience of the limb, as evidenced by the existence of congenital phantom limbs. Individuals born without an arm or leg, who have never received afferent input from the missing limb and possess no sensorimotor memory of it, nonetheless report rich phantom experiences like a hand that gesticulates during conversation and fingers that flex when the person reaches for a cup.
Ronald Melzack interpreted these cases through his neuromatrix theory, arguing that the brain possesses an innate, genetically specified body schema that exists before and independent of sensory experience. Incoming signals sculpt and refine this schema across development, but they do not create it from scratch, and in the absence of any input at all, the schema still generates a body, phantom fingers and all. The presence and functionality of a body, in this framework, is a Bayesian prior that is merely updated.
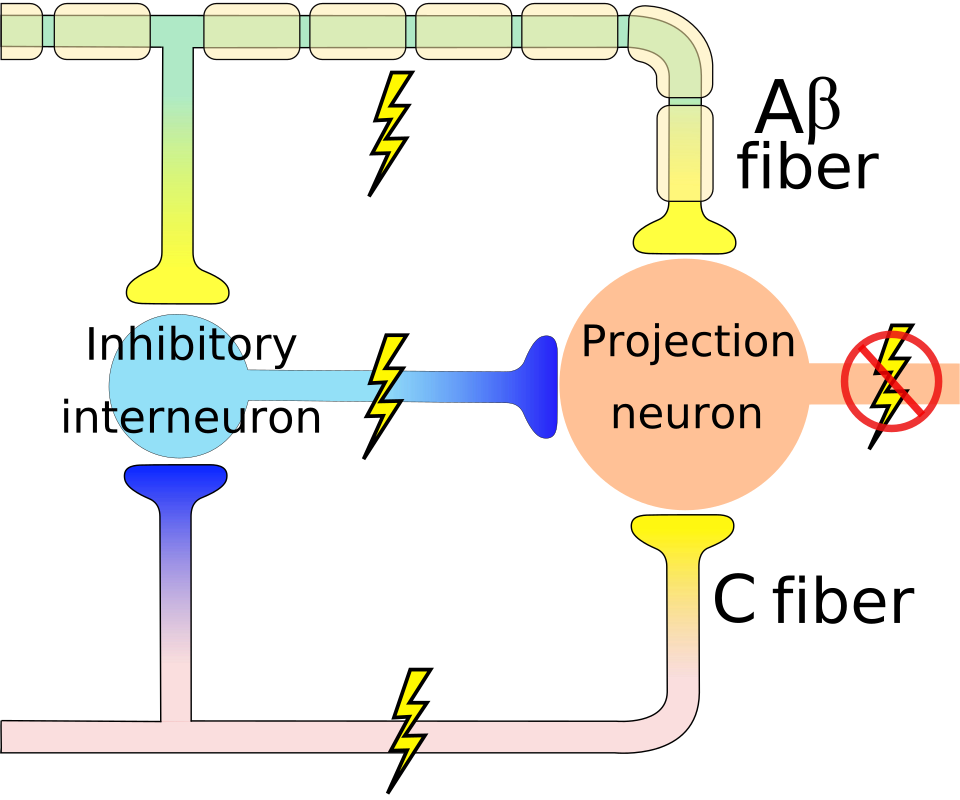
Schematic of Melzack and Wall’s gate-control theory: large myelinated afferents activate an inhibitory interneuron in the dorsal horn, closing the “gate” to nociceptive small-fiber signals before they reach the brain. Image by Delldot, licensed under CC BY-SA 3.0.
Bidirectional Brain-Computer Interfaces and Prosthetic Embodiment
This principle has become the foundation of modern neural prosthetics. Because cortical limb representations survive amputation, electrode arrays implanted in the primary motor cortex can decode intended hand movements from neural populations that have not driven a physical hand in years, and the fidelity of that decoding improves substantially when the prosthetic delivers somatosensory feedback through intracortical microstimulation of the old somatosensory maps. Users who receive this closed-loop feedback not only control the prosthetic better; they begin to embody it, reporting that the robotic hand feels like their own rather than a tool attached to their body. The ghost in the machine, it turns out, is willing to adopt a new machine.

Robotic prosthetic hand used to illustrate modern neuroprosthetic systems. Photo by uwnews/Matt Hagen, licensed under CC BY 2.0.
The malleability of the body map exposes the general principle that embodiment is a central inference. It suggests that the brain’s model of the body operates with a degree of autonomy from the physical body that should unsettle comfortable assumptions about where “the self” resides. This raises broader questions: if the brain can remap the representation of the body, can it also change to incorporate external objects? Tool-use studies show that a well-practiced rake or tennis racket briefly expands the brain’s body representation to include the implement, and virtual-reality platforms take this further. Full-body avatars and immersive games already let users “inhabit” digital bodies, and VR-based therapies extend the mirror-box principle, allowing patients to rehearse pain-free movement in simulated worlds or even to embody entirely new limbs.
Phantom limbs reveal a paradox which lies at the heart of selfhood: the brain’s map is both astonishingly plastic, capable of rewiring after catastrophes, and stubbornly conservative, clinging to a body plan that no longer matches one’s physical reality. Understanding this interplay is yielding better therapies today and, perhaps tomorrow, seamless integration between biological bodies and the machines that may one day extend them. The phantom limb, once a medical curiosity, has become a window into how the brain constructs the very idea of “me.”
References
- Paré, A. (1564). Dix livres de la chirurgie. WorldCat
- Schott G. D. (2014). Revealing the invisible: the paradox of picturing a phantom limb. Brain: a journal of neurology, 137(Pt 3), 960–969. https://doi.org/10.1093/brain/awt244
- Penfield, W. & Boldrey, E. (1937). Somatic motor and sensory representation in the cerebral cortex of man as studied by electrical stimulation. Brain, 60(4), 389–443. https://doi.org/10.1093/brain/60.4.389
- Penfield, W., & Rasmussen, T. (1950). The cerebral cortex of man: A clinical study of localization of function. Macmillan.
- Ramachandran, V. S. & Hirstein, W. (1998). The perception of phantom limbs: The D. O. Hebb lecture. Brain, 121(9), 1603–1630. https://doi.org/10.1093/brain/121.9.1603
- Pons, T. P. et al. (1991). Massive cortical reorganization after sensory deafferentation in adult macaques. Science, 252(5014), 1857–1860. https://doi.org/10.1126/science.1843843
- Flor, H. et al. (1995). Phantom-limb pain as a perceptual correlate of cortical reorganization following arm amputation. Nature, 375, 482–484. https://doi.org/10.1038/375482a0
- Faure, C., Limballe, A., & Kerhervé, H. A. (2019). Fooling the Brain, Fooling the Pain: The Role of Mirror Therapy and Modern Uses in Virtual Reality. Frontiers for Young Minds, 7. https://doi.org/10.3389/frym.2019.00091
- Ramachandran, V. S. & Rogers-Ramachandran, D. (1996). Synaesthesia in phantom limbs induced with mirrors. Proceedings of the Royal Society B, 263(1369), 377–386. https://doi.org/10.1098/rspb.1996.0058
- Melzack, R. (1990). Phantom limbs and the concept of a neuromatrix. Trends in Neurosciences, 13(3), 88–92. https://doi.org/10.1016/0166-2236(90)90179-E
- Delldot. (2008). Gate control A firing [Illustration]. Wikimedia Commons. https://commons.wikimedia.org/wiki/File:Gate_control_A_firing.svg
- Flesher, S. N. et al. (2021). A brain-computer interface that evokes tactile sensations improves robotic arm control. Science, 372(6544), 831–836. https://doi.org/10.1126/science.abd0380
- Osborn, L. E., Ding, K., Hays, M. A., Bose, R., Iskarous, M. M., Dragomir, A., Tayeb, Z., Lévay, G. M., Hunt, C. L., Cheng, G., Armiger, R. S., Bezerianos, A., Fifer, M. S., & Thakor, N. V. (2020). Sensory stimulation enhances phantom limb perception and movement decoding. Journal of neural engineering, 17(5), 056006. https://doi.org/10.1088/1741-2552/abb861
- Eck, J., & Pfister, R. (2025). Bound by Experience: Updating the Body Representation When Using Virtual Objects. Human factors, 67(2), 115–140. https://doi.org/10.1177/00187208241258315
- Maravita, A. & Iriki, A. (2004). Tools for the body (schema). Trends in Cognitive Sciences, 8(2), 79–86. https://doi.org/10.1016/j.tics.2003.12.008
- Cardinali, L. et al. (2009). Tool-use induces morphological updating of the body schema. Current Biology, 19(12), R478–R479. https://doi.org/10.1016/j.cub.2009.05.009

{kind=link}